
SNAP Cuts Add to States’ Mounting Fiscal Pressures
Seemingly at odds with the MAHA agenda, changes to SNAP eligibility and cost sharing will put extra pressure on states to fill food assistance gaps — or reduce resources for the SNAP program.

Author: Cindy Long
Editors: Patti Boozang and Amanda Eisenberg
tl;dr
H.R.1 has made sweeping changes to the Supplemental Nutrition Assistance Program (SNAP), including expanding program work reporting requirements, narrowing eligibility for certain non-citizens, eliminating over $500 million in food education programs and shifting costs from the federal government to states.
With about $186 billion in SNAP cuts over the next decade, more than 22 million households receiving food assistance could experience greater food insecurity — and state Medicaid agencies could feel the ripple effects.
Historically, states have not been obligated to fund SNAP benefits. The federal government paid 100% of benefit costs and 50% of administrative costs, with state and local governments taking up the balance of administration. H.R.1 fundamentally changes this arrangement by requiring states and local governments to take on more of the cost of administering the program and, for the first time in SNAP history, requiring states to fund part of benefit payments if their payment error rate is 6% or more, according to the according to the U.S. Department of Agriculture’s Food and Nutrition Service (FNS).
The potential fiscal impact to states is enormous, bringing new uncertainty about whether states will trim their SNAP programs.
The 80 Million Impact
While we have focused primarily on H.R.1 changes to health coverage, the law brings other significant changes to health and human services benefits that impact state budgets, compounding Medicaid funding cuts, and the health and wellbeing of state residents including Medicaid enrollees. H.R.1 makes $186 billion in cuts to SNAP over the next decade through a series of key policy changes. These changes drive seismic funding and administrative changes in the short term and Medicaid enrollee health status and cost of care impacts in the longer term.
SNAP provides households with subsidies that help them meet their basic food needs. Good nutrition is essential to tackling foundational drivers of chronic health conditions that plague many Americans, including diabetes, high blood pressure, and obesity. Indeed, the MAHA agenda has focused on childhood obesity, food quality, and the elimination of ultra-processed foods from American diets. And for states thinking about the rapid growth of their pharmaceutical, emergency care, and acute care costs in Medicaid, the prospect of families losing access to affordable food is deeply troubling.
Ashleigh Ligon, a mother of six who lives in Seattle, told The 80 Million she relies on SNAP to feed her family. Her 6-year-old son has severe food allergies, which means she needs to prioritize his dietary restrictions — sometimes at the sake of the rest of her family’s dietary needs.
“I have so much fear, I have so much worry,” she said. “If I’m not eligible for Medicaid or SNAP, there will be a serious issue feeding my children. My adult son, my husband and I will not be able to eat enough. [The younger kids] will not be able to eat in the same way they do now. It’ll break my heart to tell my kids they can’t have seconds.”
Ligon’s sons also attend cooking classes in their community — the type of program that could also disappear with the loss of $500 million in annual food education funding, which took effect on Sept. 30.
Expanded Work Requirements
H.R.1 tightens SNAP work requirements, expanding mandatory participation to adults ages 18–64 and parents or caregivers whose youngest child is 14 or older. The bill also removes previous SNAP work requirement exemptions for veterans, people experiencing homelessness, and youth aging out of foster care, while making it much harder for states to waive these rules. About 1.5 million people may lose access to SNAP if they can’t report their work hours, according to the Center on Budget and Policy Priorities. States will be expected to implement work reporting requirements for Medicaid starting in January 2027, which will increase the administrative burden and complexity of determining exemptions from and compliance with work requirements across Medicaid and SNAP.
Benefits Cost Shift to States
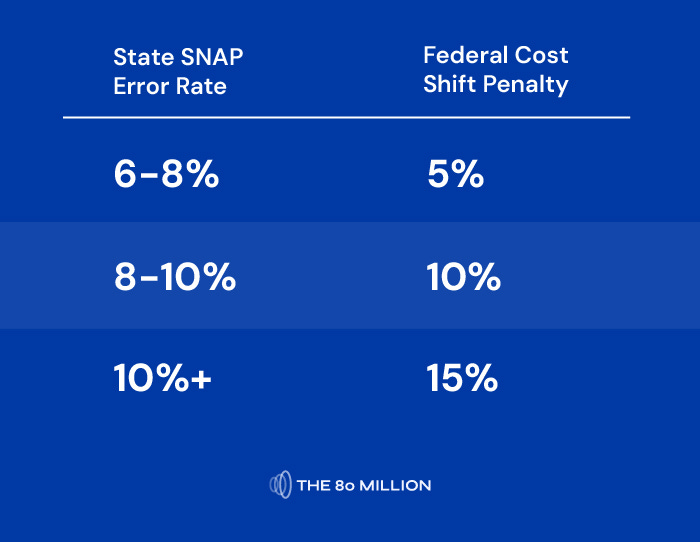
H.R.1 includes two historic cost shifts to states, impacting both benefits and administrative costs. Starting in FY 2028, states with payment error rates above 6% must pay 5%-15% of the costs of SNAP. This is designed to incentivize states to improve accuracy of their eligibility and benefit determinations — a theoretically reasonable goal, but one that risks catastrophic results. It is not at all clear that all states can achieve this standard in this timeframe or at all. Indeed, as program eligibility for SNAP becomes more complex, it becomes harder for states to administer with accuracy. Further, things like eligibility documentation mistakes for people who are eligible are often counted as “eligibility errors” driving up state error rates. States also currently face staffing shortages and IT system constraints that will be far more challenging to address with the SNAP funding cost shift from the federal government to state and local governments.
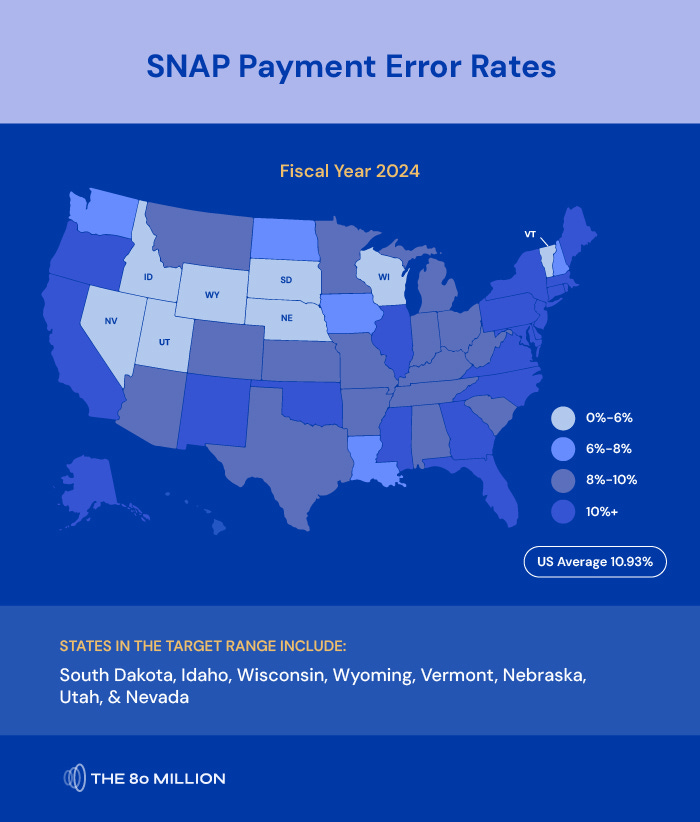
Notably, just eight states — Idaho, Nebraska, Nevada, South Dakota, Utah, Vermont, Wisconsin, and Wyoming — had SNAP error rates below the 6% threshold last year, according to FNS. The national payment average error rate for fiscal year (FY) 2024 was 10.93%, per FNS. So, most states stand to be deeply impacted by the fiscal implications of the new H.R.1 SNAP policies.
States who are unable to achieve the target will be liable for added benefit costs, totaling in the hundreds of millions in many states. States who are unable or unwilling to provide these funds will face an unprecedented choice — either find ways to dramatically reduce caseload through restrictive policy and operational choices (while still meeting federal eligibility and benefit requirements) or opt out of the program entirely.
Administrative Cost Shift to States
Starting in FY 2027, states will be required to shoulder 75% of administrative costs for SNAP, compared to a 50-50 split between federal and state governments today. States will need to devote scarce resources simply to maintain the status quo. Providing the additional investments needed to reduce error rates and implement other changes required by H.R.1 will be even more challenging. While new technologies may offer opportunities for improving cost efficiency, the increased funding burden will likely result in service deterioration — particularly in the near term — and incentivize states to consider reducing or dropping the program altogether.
These dramatic reductions to nutrition assistance funding put the food security — and thus health — of millions of lower-income Americans at risk, making diet-related disease prevention significantly more challenging.
The Bottom Line
The changes to SNAP under H.R.1 represent a seismic shift in how nutrition assistance is funded and administered in the United States. By transferring unprecedented financial and operational burdens to states — while simultaneously narrowing eligibility and expanding work requirements — these policies risk destabilizing a program that millions rely on for basic food security. Compounding these changes in the short term, the government shutdown will likely bring further disruption to SNAP. The USDA told states that there won’t be sufficient funds available in November and that until further notice, they shouldn’t take any steps to load benefit cards. If benefits are halted, it would be unprecedented and have a deleterious impact on the 40+ million individuals who rely on SNAP.
Looking ahead, states now face the dual challenge of absorbing hundreds of millions in new SNAP costs and navigating complex compliance requirements, all while confronting staffing shortages and outdated systems. The ripple effects will be felt not only in state budgets, but in the health and wellbeing of vulnerable families, with Medicaid agencies bracing for increased costs as food insecurity rises.